If you or a patient is in crisis: Call or text 988 (Suicide and Crisis Lifeline) or visit 988lifeline.org
This article outlines the partnership between BestNotes and SPiER (Suicide Prevention, Intervention, and Education Resources) to integrate evidence-based suicide prevention workflows into your EHR, providing tools and protocols for suicide-safer patient care.
Permissions Required
No specific BestNotes permissions are required.
Implementing the Suicide-Safer Care Pathway with SPiER
BestNotes has partnered with SPiER (Suicide Prevention, Intervention, and Education Resources) to embed evidence-based suicide prevention workflows directly into your clinical documentation — at no additional cost. The collaboration brings together BestNotes' commitment to patient-centered care with SPiER's implementation-focused work translating suicide-safer care practices into practical workflows, structured documentation, and technology-enabled supports — fulfilling BestNotes' founding promise to Help the Helper™.
What's Included
- Embedded risk screeners — Automated prompts for the C-SSRS and ASQ surfaced at the right moment in clinical documentation.
- Digital safety planning — Structured Stanley-Brown Safety Plan templates co-created with patients — stored as structured data, not a PDF.
- Clinical decision support (CDS) — Automatic prompts for lethal means counseling, psychiatric referrals, and other interventions when a patient's screener score indicates elevated risk. Standardized risk flags — Visual alerts in the patient chart, visible to care teams across departments during handoffs.
- Caring contacts — Automated post-visit follow-up surveys to maintain engagement with at-risk individuals after they leave the care setting.
- Education & training resources — Access to SPiER training and awareness materials through OutcomeTools.
Collaborative Care Management (COCM) Suicide-Safer Care Pathway Steps
The pathway begins with universal PHQ-9 screening at every primary care contact. When a patient answers yes to item 9, or suicidal thoughts/behavior are otherwise identified, the C-SSRS with Triage Points is administered. The score determines the patient's risk tier and required care.
- Universal Screening
All patients receive universal PHQ-9 screening in primary care. If YES to Q9 (or suicidal thoughts/behavior identified with clinical judgement), proceed to C-SSRS. If the patient scores "No" on all C-SSRS questions, they do not enter the pathway.
Step 2: Risk Tier Identification
The following table outlines the criteria for identifying risk tiers:
Step 3: Care Requirements by Risk Level
H Historical risk
- Provide 988 crisis resources and NowMattersNow.org
- Provide Emotional Fire Safety Plan
- Reassess C-SSRS prior to discharge (or more frequently as clinically indicated)
- Add Z91.82 (History of Suicidal Behavior) or Z91.5 (History of Suicide Attempt) to problem list
- Psychiatric: Full Safety Review at next scheduled consult
- Patient contact: as clinically indicated
L Low risk
- Provide 988 crisis resources and Emotional Fire Safety Plan
- Reassess C-SSRS every 30 days (or more frequently as clinically indicated)
- Add R45.851 (Suicidal Ideation) to problem list
- Psychiatric: Full Safety Review at next contact, then monthly
- Patient contact: at least every month
M Moderate risk
- Provide 988 crisis resources and Emotional Fire Safety Plan
- Complete Stanley-Brown Safety Plan and obtain consent for engaging emergency contact; review and modify at each contact
- Reassess C-SSRS every 14 days (or more frequently as clinically indicated)
- Add R45.851 to problem list
- Psychiatric: Full Safety Review at next contact, then every 14 days
- Patient contact: at least every 14 days
H High risk
- Provide 988 crisis resources and Emotional Fire Safety Plan
- Complete Stanley-Brown Safety Plan and obtain consent for engaging emergency contact; review and modify at each contact
- Add R45.851 to problem list
- Psychiatric: Full Safety Review at next contact, then every 7 days
- Patient contact: at least every 7 days
Missed Appointments Protocol
If a patient at any risk level misses or no-shows a scheduled appointment, follow these steps at every contact:
- Ask C-SSRS-SLC+ Q6 immediately
"Are you having thoughts of killing yourself right now?" — administer at the time of contact. - Revise the safety plan
Update the Stanley-Brown Safety Plan based on current presentation and changes since last contact. - Complete clinical assessment including full C-SSRS
Re-establish current risk level with a full clinical assessment. - Consider alternate level of care
Counsel patient on lethal means reduction. Assess immediate supports. Consult supervisor if possible. Consider wellness check before end of day. Alert care team. - Call immediately at time of contact
Do not wait — reach out to the patient within the hour. Consider outreach to emergency or safety plan contacts if the patient cannot be reached.
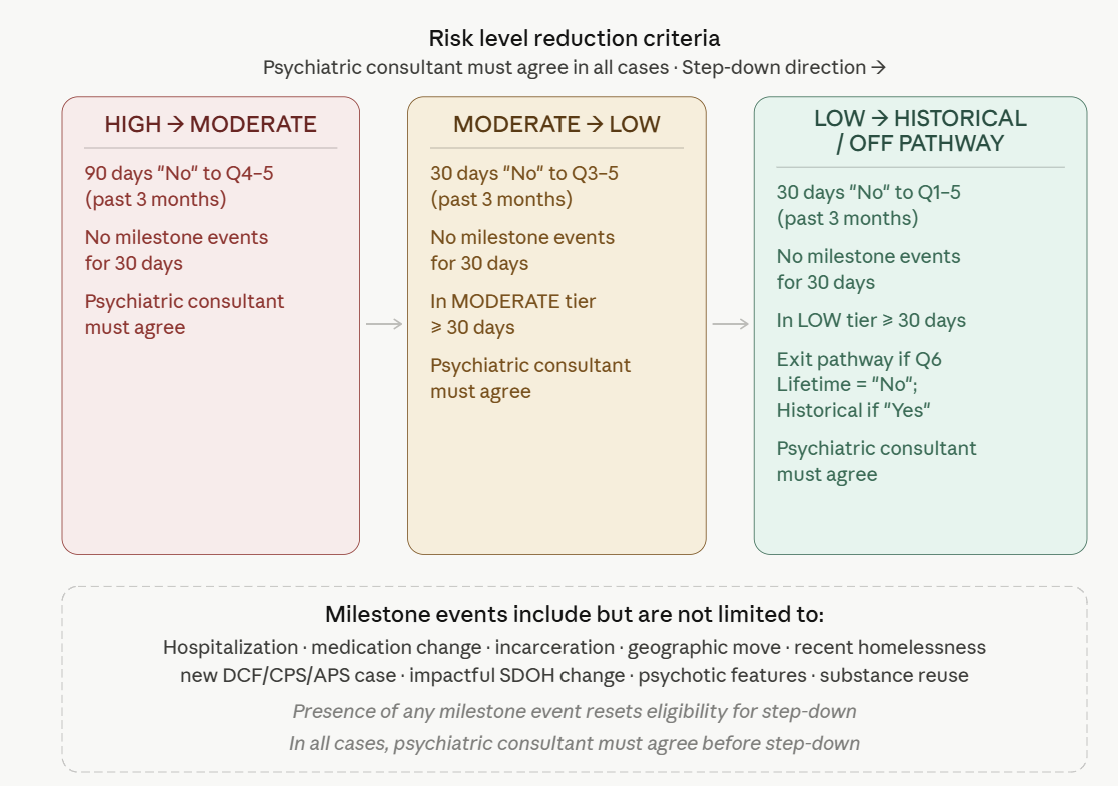
Risk Level Reduction Criteria
Patients may step down to a lower risk tier when all criteria below are met.
Quality Measures Tracked
- PHQ-9 Q9 follow-through rate % of patients with a positive PHQ-9 Q9 response who receive a C-SSRS Screen with Triage Points.
- C-SSRS documentation rate % of patients with a positive C-SSRS screen who have a suicide-related entry added to the problem list and a risk flag in the chart.
- Safety plan provision rate % of patients in each risk tier who were provided the appropriate safety plan or crisis resources.
Frequently Asked Questions
Is there an additional cost for SPiER features?
No. SPiER workflows, education resources, and clinical tools are included for all BestNotes customers at no additional cost.
When is this available?
The partnership is effective June 2026. EHR workflow capabilities are available to all BestNotes customers beginning June 2026. Existing customers will receive an email with instructions to transition their OutcomeTools account.
Does the safety plan follow the patient across care settings?
Yes. BestNotes clinical workflows are built on HL7 FHIR interoperability standards. Risk assessments, safety plans, and risk flags are stored as structured, portable data that travels securely with the patient across settings.
How does this support the Zero Suicide Initiative?
SPiER provides the technological and educational infrastructure to implement Zero Suicide consistently — making suicide-safer care measurable and standardized, not dependent on individual clinician habits.
Where do I access SPiER education resources?
SPiER resources are available through OutcomeTools. Details will be shared with customers upon rollout. You can also submit a support ticket for direct support.
Does this work across different care settings?
Yes. Because SPiER is built on HL7 FHIR standards, a patient's safety plan and risk indicators are no longer siloed — information follows the patient securely during care transitions.
Next Steps
- Submit a support ticket for direct assistance.
- Visit the BestNotes website: bestnotes.com
- Learn more about the SPiER project: theSPiERproject.org
- Access crisis resources: 988lifeline.org
This is a suggested pathway for assisting organizations in developing their own guidelines in congruence with local, state, and organizational policies and regulatory requirements. Care pathway developed by Tej Carbone and Dr. Virna Little. © 2022 NCT Consulting. All Rights Reserved.
Back to top of page